 Lu Zang1
Lu Zang1 Chunliang Cheng
Chunliang Cheng Xuemei Liu
Xuemei Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 06 January 2023
Sec. Psycho-Oncology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.1028934
Introduction: The study aimed to investigate the effect of music therapy on anxiety alleviation among cancer patients.
Methods: A comprehensive literature research was performed in four electronic databases (PubMed, Embase, Cochrane Library, and Web of Science). Fifteen randomized controlled trials (RCTs) were included. The risk of bias for the RCTs was evaluated by the Cochrane Risk of Bias tool. Anxiety levels were extracted to synthesize the combined effect by using meta-analysis. All analyses were performed using R version 4.0.4.
Results: In total, 15 RCTs met the inclusion criteria involving 1320 cancer patients (662 patients in the experimental group and 658 patients in the controlled group). The majority of interventions were performed with recorded music lasting for 15-60 minutes. Compared with standard care, music intervention had a moderate superiority of anxiety alleviation (SMD: –0.54, 95% CI: [–0.92, –0.16]).
Discussion: Music intervention could reduce cancer-related anxiety moderately. Nevertheless, the result should be interpreted with caution as high heterogeneity in this pooled study. Well-designed trials with higher quality were still warranted in the future.
Anxiety symptom was remarkably common in cancer survivors. Approximately, 19.0% of patients with cancer suffered from clinical levels of anxiety and 22.6% had subclinical symptoms (Linden et al., 2012). The diagnosis of cancer often tremendously increased the risk of anxiety and impacts patients’ mental health and quality of life (Lee et al., 2021). Clinically, the procedure of cancer diagnosis and treatment also caused anxiety. The discomfort and complication of this procedure would increase the psychological burden. Besides, anxiety in individuals with cancer would increase the possibility of a visit to the emergency department, the length of hospitalizations, and healthcare costs (Mausbach et al., 2020). Thus, patients with cancer with anxiety had a significantly higher risk of cancer-specific mortality and all-cause mortality (Wang et al., 2020). It was important for the clinician to be concerned about anxiety in the routine clinical practice and provide psychosocial support for patients with cancer.
In recent years, several non-pharmacological interventions reported a positive effect in alleviating treatment-related anxiety (Tola et al., 2021). Among them, music therapy was used to relieve depression (Zhao et al., 2016), Alzheimer’s disease (Giovagnoli et al., 2017), and postoperative pain (Simavli et al., 2014). It can be performed in two main forms with the monitoring of a clinician—active and receptive treatments. Active music therapy enabled patients to forwardly participate in the creation of music via singing or playing musical instruments. Conversely, receptive music therapy referred to passively listening to live music or recorded music selected by the clinician or the patient. Active music therapy involved multisensory stimulation mainly in the form of teamwork and contributed to patients’ cognition, mood, quality of life, and other aspects (Pacchetti et al., 2000; Wu et al., 2022). By contrast, receptive music therapy was more available and easier to implement in hospitals. The pace and melody of music would distract patients from clinical procedure—most of which were potentially invasive and painful, such as biopsy, operation, chemotherapy, or radiation therapy in the management of cancer.
For these reasons, several randomized controlled trials were carried out to assess the effect of receptive music therapy on anxiety reduction in routine cancer management. To date, the effect of music therapy on anxiety reduction was still inconclusive. The majority of these RCTs demonstrated a positive effect (Shabanloei et al., 2010; Li et al., 2012; Chen et al., 2013), while other RCTs revealed no significant impact on anxiety reduction. The study of Kwekkeboom (2003) showed that the effects of music and standard care, as usual, were equivocal, which was not sufficiently convincing of the limited sample size and diverse clinical procedures. Wren et al. (2019) was a three-arm clinical trial, and the defect of this study was also the limited sample size in each arm. In addition, O’Steen et al. (2021) demonstrated that music therapy did not reduce anxiety to a meaningful degree during radiation therapy. Whereas subsequent RCTs found music therapy a positive effect during radiation therapy (Chen et al., 2013; Rossetti et al., 2017). And meta-analysis review to combine these results is scarce in the literature. Therefore, this study attempted to address this research gap to provide high-quality evidence for this aspect.
The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). In May 2022, a comprehensive literature search was performed in four online electronic databases (PubMed, Embase, Cochrane Library, and Web of Science). The start time in the search was restricted to the last 30 years (i.e., 1993–2022). The language of the literature was limited to English. Additionally, available literature from other published meta-analysis were also extracted.
The procedure of literature inclusion was in accordance with the PICOS principle, including (1) Population: Adults (≥18 years) who were diagnosed with solid tumors or hematologic malignancies and/or received adjuvant therapy (chemotherapy, radiation therapy, and immunotherapy) in the potential studies; (2) Intervention: The experimental group who received music therapy and routine treatment; (3) Comparison: The controlled group was treated with routine treatment without music therapy; (4) Outcomes: The level of post-test score in anxiety or anxiety score changes which is defined as post-treatment anxiety minus pre-treatment anxiety measured by the State-Trait Anxiety Inventory (STAI); and (5) Study design: Only randomized controlled trial and high-quality quasi-experimental studies were included. We excluded patients who underwent biopsy or operation for diagnostic purposes and those with palliative treatment. Studies exhibiting no post-test score or score change in the full text would also be excluded.
Two researchers were independently assigned to screen some pieces of literature for identifying potential studies according to the inclusion criteria. Any conflicts in study selection would resort in the third researcher’s judgment. Duplicates were excluded by Endnote X9 software and manual selection. Then researchers screened the title and abstract of passages independently. Any unsuitable types such as reviews, meta-analyses, case reports, short surveys, editorials, letters, laboratory studies, or articles not related to the inclusion criteria would be further excluded. Finally, the full-text articles were obtained and evaluated for final determination. The detailed flow for literature screening is shown in Figure 1. Notably, we included Danhauer et al. with caution for the consideration that bone marrow biopsy in this trial was not performed for diagnostic purposes but served as a routine monitor of treatment.

Figure 1. The flow for literature screening.
The general information for the included studies was extracted using a predesigned Excel sheet, which included the first authors’ name, publication year, country, patients’ age, gender distribution, and sample size. Cancer type, intervention in the experimental group, treatment in the controlled group, the procedure and duration of music therapy, scale for outcome measurement, and study result were also extracted.
The quality of the included literature was assessed by the Cochrane Risk of Bias tool (Higgins et al., 2011). Two researchers independently evaluated the potential bias of RCTs in the seven aspects: “random sequence generation,” “allocation concealment,” “blinding of participants and personnel,” “blinding of outcome assessment,” “incomplete outcome data,” “selective reporting,” and “other bias.” According to the full-text articles, researchers marked these aspects with low, high, or unclear risk of bias. If there were any disagreements in bias assessment, they would be discussed with the third researcher.
The present analysis was performed to identify the effect of music therapy on alleviating cancer-related anxiety. The level of the post-test score and score change were continuous variables given as means ± standard deviations (SD). Cochran’s Q test was used to identify the heterogeneity of results by I square (I2 < 25%: no heterogeneity; I2 = 25–50%: moderate heterogeneity; I2 > 50%: large heterogeneity). If I2 < 50%, the fixed effects model was applied. The random-effects model was adopted if I2 ≥ 50%, which indicated homogeneous results between included studies (Higgins and Thompson, 2002). Publication bias was visualized by funnel plot. Sensitivity analysis was made by reducing one literature at a time until the heterogeneity was low. A two-sided P-value of <0.05 was considered as the threshold of statistical significance. All analysis and figure generation were performed using R version 4.0.4.
In total, 15 RCTs (Kwekkeboom, 2003; Bulfone et al., 2009; Danhauer et al., 2010; Lin et al., 2011; Li et al., 2012; O’Callaghan et al., 2012; Chen et al., 2013; Vachiramon et al., 2013; Zhou et al., 2015; Alam et al., 2016; Firmeza et al., 2017; Rossetti et al., 2017; Wren et al., 2019; Al-Jubouri et al., 2021; Mishra et al., 2022) were included in the present analysis involving 1,320 patients with cancer (Table 1). Among these trials, the majority of them (7/15) were conducted in America (Kwekkeboom, 2003; Danhauer et al., 2010; Vachiramon et al., 2013; Alam et al., 2016; Rossetti et al., 2017; Wren et al., 2019; Mishra et al., 2022), followed by four in China (Lin et al., 2011; Li et al., 2012; Chen et al., 2013; Zhou et al., 2015), one in Italy (Bulfone et al., 2009), one in Iraq (Al-Jubouri et al., 2021), one in Australia (O’Callaghan et al., 2012), and one in Brazil (Firmeza et al., 2017). Four studies included patients who had been diagnosed with breast cancer (Bulfone et al., 2009; Li et al., 2012; Zhou et al., 2015; Wren et al., 2019), two studies included patients with skin cancer (Vachiramon et al., 2013; Alam et al., 2016), one study included patients with prostate cancer (Mishra et al., 2022), one study included hematological malignancies (Danhauer et al., 2010), and one study included patients with head and neck cancer (Firmeza et al., 2017). For the rest of the studies, mixed group of cancer patients were included (Kwekkeboom, 2003; Lin et al., 2011; O’Callaghan et al., 2012; Chen et al., 2013; Rossetti et al., 2017; Al-Jubouri et al., 2021). Of all the selected trials, 662 patients underwent music therapy with routine treatment, while 658 patients received only the routine treatment. Three studies (Table 2) were performed to decrease chemotherapy-related anxiety (Bulfone et al., 2009; Lin et al., 2011; Al-Jubouri et al., 2021). Three were performed for radiotherapy-related anxiety alleviation (O’Callaghan et al., 2012; Chen et al., 2013; Rossetti et al., 2017). Eight were designed for mitigating anxiety during surgery (Kwekkeboom, 2003; Danhauer et al., 2010; Li et al., 2012; Vachiramon et al., 2013; Zhou et al., 2015; Alam et al., 2016; Wren et al., 2019; Mishra et al., 2022). Five trials demonstrated its study results with anxiety changes (O’Callaghan et al., 2012; Chen et al., 2013; Alam et al., 2016; Firmeza et al., 2017; Rossetti et al., 2017), while 11 trials only exhibited post-treatment anxiety in the full text (Kwekkeboom, 2003; Bulfone et al., 2009; Danhauer et al., 2010; Lin et al., 2011; Li et al., 2012; O’Callaghan et al., 2012; Vachiramon et al., 2013; Zhou et al., 2015; Wren et al., 2019; Al-Jubouri et al., 2021; Mishra et al., 2022). All the outcomes were measured by STAI.

Table 1. The characteristics of included studies.
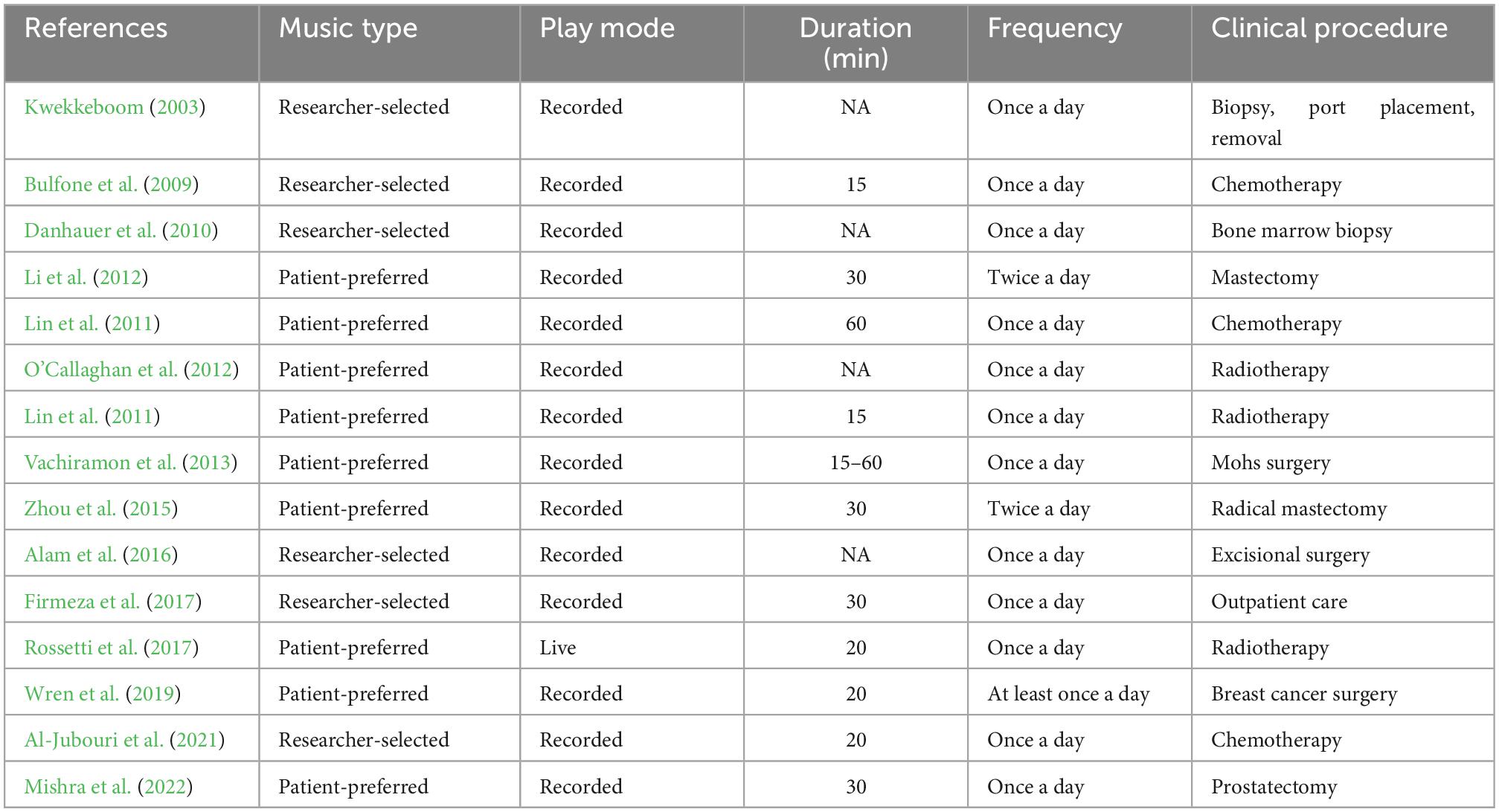
Table 2. The details of music intervention.
The risk of bias assessment result is shown in Figure 2. Two trials did not report the randomized allocation in the procedure, thus allocation concealment was also considered as “high risk,” as they did not display the randomization procession method. As the performance bias was not avoided for music therapy, all 15 trials were deemed as “unclear risk” in the blinding of participants and personnel. The detection bias was unclear for all trials. Thirteen trials reported attrition (dropout of participants) in the experiment, and they were evaluated as “low risk” in the attrition bias aspect. No reporting and other biases were observed in all trials.

Figure 2. Risk of bias assessment for 15 included studies.
Eight trials reported the anxiety score in post-treatment measured by STAI. No significant difference in anxiety baseline was observed in these trials before the music therapy was performed. As high heterogeneity was observed (I2 = 68%), the random effects model was applied to the analysis. The meta-analysis (Figure 3A) showed a positive combined effect in favor of music therapy (SMD: −0.54, 95% CI: [−0.92, −0.16], I2 = 87%). Sensitivity analysis (Figure 3B) indicated that the three studies extremely affected the overall heterogeneity. By omitting these studies, low heterogeneity was observed. In addition, the pooled effect of music invention was moderate (SMD: −0.66, 95% CI: [−0.86, −0.46], I2 = 36%).
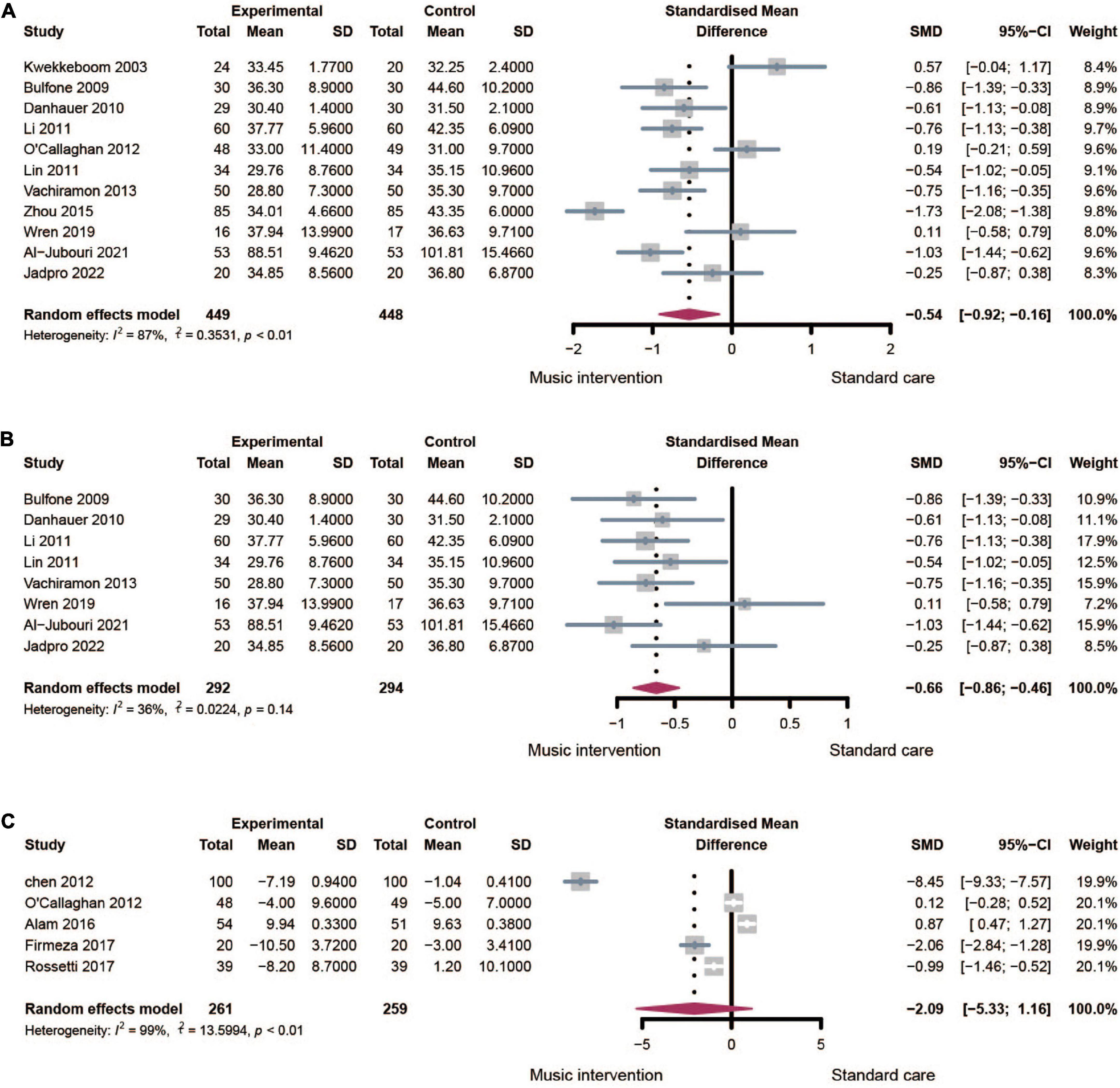
Figure 3. Forest plots for music therapy on anxiety. (A) Effect of music therapy measured by post-treatment anxiety with high heterogeneity. (B) Effect of music on therapy measured by post-treatment anxiety after sensitivity analysis. (C) Effect of music on therapy measured by anxiety changes.
Five trials displayed anxiety score changes measured by STAI. A random-effects model was performed as the high heterogeneity (I2 = 99%) in the analysis. The meta-analysis (Figure 3C) demonstrated that music therapy could alleviate anxiety in patients with cancer (SMD: −2.09, 95% CI: [−5.33, −1.16]). Sensitivity analysis indicated that high heterogeneity was unavoidable by omitting any one trial. Moreover, given the limited trial number, subgroup analysis was not suitable.
The subgroup analysis of gender distribution was displayed in Figure 4. Studies could be divided into the female, male, and mixed groups in association with gender. Considering there was only one study in the male group, we compared the female and mixed groups in the below analysis. The effect of music therapy in the mixed group was calculated with an SMD of −0.38 (95% CI: [−0.85, 0.10], I2 = 84%). Whereas, a greater effect was calculated in the female group (SMD: −0.84, 95% CI: [−1.57, −0.12], I2 = 89%). Since a decrease in inter-study heterogeneity was not observed, gender distribution may not be the source of heterogeneity.
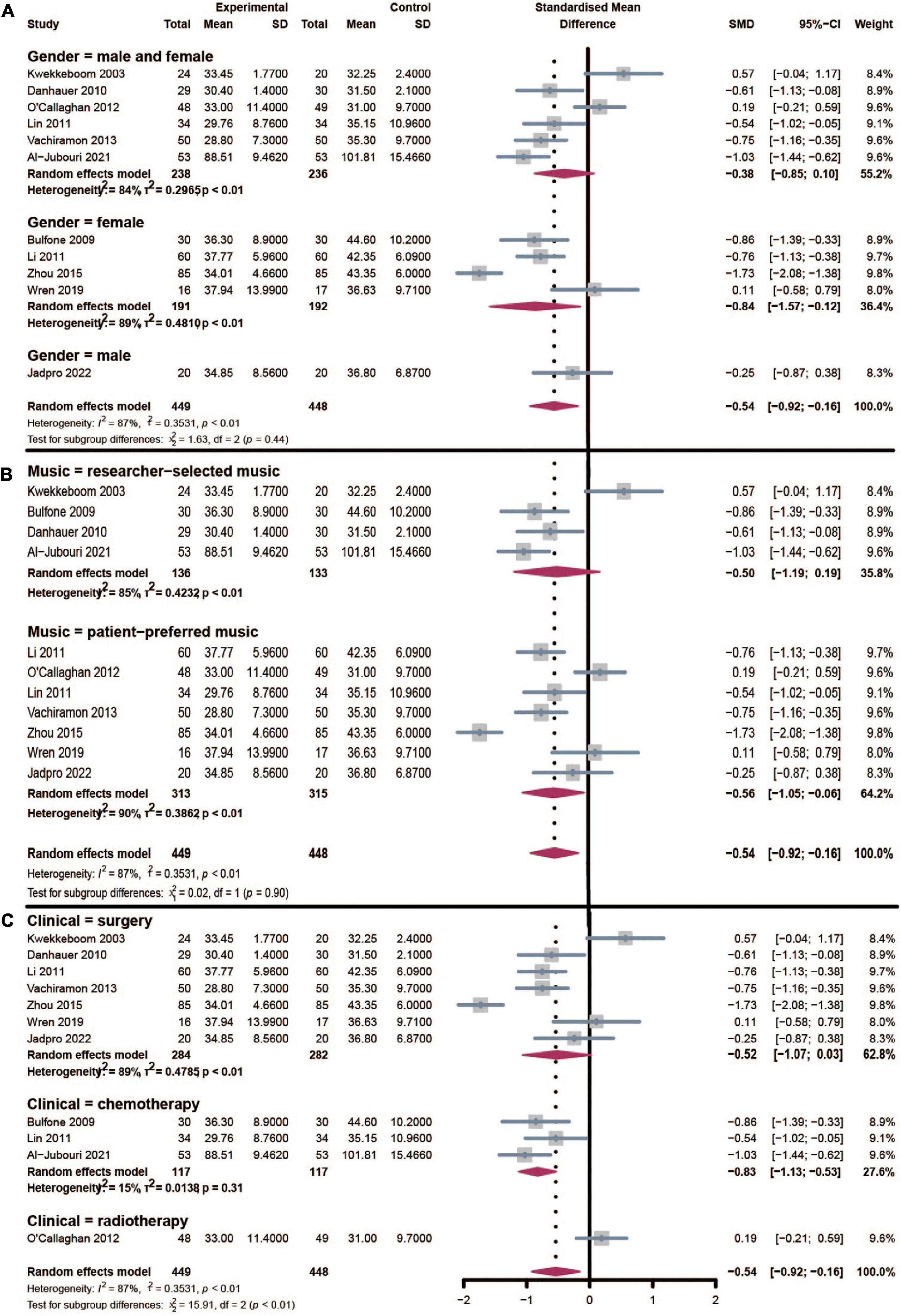
Figure 4. Subgroup analysis of the effect of music therapy on gender distribution (A), music type (B), and clinical procedure (C).
According to the music type provided to patients with cancer, studies could also be divided into researcher-selected music, and patient-preferred music groups (Figure 4B). Music therapy could significantly reduce treatment-related anxiety in the researcher-selected music group (SMD: −0.50, 95% CI: [−1.19, 0.19], I2 = 85%). And patient-preferred music offered a similar positive effect in anxiety reduction (SMD: −0.56, 95% CI: [−1.05, −0.06], I2 = 90%). Similarly, the inter-study heterogeneity was still high in these groups, and music type was not a potential moderator variable that caused heterogeneity.
All the included studies were performed to explore the effect of music therapy in reducing treatment-related anxiety. These clinical procedures included surgery, chemotherapy, and radiotherapy (Figure 4C). Music intervention could significantly alleviate surgery-related anxiety with an SMD of −0.52 (95% CI: [−1.07, 0.03], I2 = 89%). Whereas, music would have a greater effect in reducing chemotherapy-related anxiety (SMD: −0.83, 95% CI: [−1.13, −0.53], I2 = 15%) with a much lower heterogeneity. These factors indicated that clinical procedure was mainly or partly the source of heterogeneity. As only one study was in the radiotherapy group, subgroup analysis was not available for it.
Four studies were performed among patients with breast cancer. Music therapy (Supplementary Figure 1) could significantly reduce treatment-related anxiety in breast patients with breast cancer (SMD: −0.84, 95% CI: [−1.57, 0.12], I2 = 89%).
The publication bias of the included studies was displayed in Supplementary Figure 2. The relatively symmetrical funnel plot indicated that there was no publication bias among all the included studies.
The effectiveness of music intervention on cancer-related anxiety is disputable. In the present study, a comprehensive literature search was performed to synthesize novel randomized controlled trials to provide high-quality evidence in this aspect. The meta-analysis results indicated the positive effect of music intervention on anxiety management during routine clinical treatment among patients with cancer covering chemotherapy, radiation therapy, and surgery without general anesthesia.
A moderate superiority of anxiety alleviation in music intervention (SMD: −0.54, 95% CI: [−0.92, −0.16]) was observed compared with standard care. Inconsistent with the initial meta-analysis published in 2013 (Nightingale et al., 2013), the result supported the positive impact of music therapy on treatment-related anxiety. The contradiction was mainly derived from the included limited studies (four RCTs). Two previous meta-analysis reviews also reported the combined effect of music on anxiety reduction. Li et al. (2020) included six RCTs with anxiety score changes as the outcome data. On the contrary, Nguyen et al. (2022) used post-test anxiety scores in another six RCTs. The drawback of these studies above was the insufficient number of included literature works. Moreover, the two previous pooled studies included diverse scales to measure the baseline and post-intervention anxiety levels, including State-Trait Anxiety Inventory State (STAI-S), the Self-Rating Anxiety Scale (SAS), and the Hospital Anxiety and Depression Scale (HADS) tests. This would lead to potential bias in the literature selection.
In the present study, we systematically searched all the relevant works of literature which reported anxiety score changes or post-test anxiety score levels. To avoid potential bias and heterogeneity, we further restricted to enroll RCTs involving adults and measured by STAI, which was commonly used for medical patients. In total, 15 randomized controlled trials were included. In our opinion, anxiety score change would be more suitable for quantifying the effect of music therapy. Although all the studies declared that the baseline anxiety level was similar (P < 0.05) between the intervention group and the controlled group. Considering diverse cancer types, various stages, gender, or age distribution in different studies, baseline anxiety levels and post-test scores were greatly discrepant among studies which would also increase potential heterogeneity in the meta-analysis. To inspire subsequent RCTs to improve experimental design, we did not exclude four studies that only displayed the anxiety score change, and they were analyzed separately. The SMD method was also used in this study to synthesize the data.
Yet, the present study observed high heterogeneity (I2 = 87%) in the data synthesis which should be interpreted with caution. Subgroup analysis was performed to seek the potential factors of high heterogeneity. A previous study reported that women and the elderly would be more likely to suffer from anxiety after diagnosis of cancer (Linden et al., 2012). In our subgroup of gender distribution, music therapy would be more effective in the female group compared with the mixed group in association with gender. It indicated that non-pharmacological interventions like music therapy were suitable for routine clinical practice. Subgroup analysis revealed that gender distribution would not affect heterogeneity in the analysis. In the subgroup analysis of music type, the performance of researcher-selected music and patient-preferred music seemed similar. More high-quality RCTs were still needed to support this conclusion. Similarly, heterogeneity was not caused by music type. In the subgroup of clinical procedure, we revealed that music therapy would be more effective in reducing chemotherapy related with low heterogeneity (I2 = 15%). It indicated that different clinical procedures in the included studies were the source of the heterogeneity. Meanwhile, we noticed high heterogeneity in the surgery group. The diverse surgery category in the included studies would be the reason such as mastectomy, prostatectomy, bone marrow biopsy, port placement, and Mohs surgery. Considering the limited number of RCTs, more specialized subgroups were not available.
To reduce high heterogeneity, sensitivity analysis was also performed. It indicated that there was low heterogeneity (I2 = 36%) when omitting the three studies (Kwekkeboom, 2003; Zhou et al., 2015; Wren et al., 2019). Besides, several factors would also impact the heterogeneity in this study. Due to the limited number of included studies, we could not use subgroup analysis to explore the potential impact of age, cancer type, cancer staging, duration of music, or frequency of intervention. All the abovementioned discrepancies would be unavoidable, leading to heterogeneity in this study. More pieces of evidence of high quality in future were needed.
In terms of risk of bias, the majority of included RCTs lacked adequate quality and were deemed high risk in the bias assessment. Two trials did not describe the allocation concealment procedure. As music inventions were not suitable for participant blindness, all the trials were considered as an unclear risk in the performance bias. None of the trials adopted blinding of outcome assessment in the experiment design. Future studies should optimize the experiment design to obtain more high-quality results.
This meta-analysis has some primary limitations: First, the number of included studies is limited which may unavoidably result in bias and high heterogeneity. Another limitation was that the quality of the included studies was moderate. Besides, unpublished studies, including “gray studies,” were not included in our meta-analysis. These factors may have a negative impact on the results of our study.
The present analysis demonstrated that music intervention could reduce cancer-related anxiety with a moderate effect. However, considering the high heterogeneity and risk of bias of the included trials, more well-performed and larger-scale RCTs are required to verify the value of music intervention in reducing anxiety among patients with cancer.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
LZ: conceptualization and writing—original draft preparation. CC: methodology and software. YZ: data curation and visualization. XL: writing—review and editing and supervision. All authors contributed to the article and approved the submitted version.
This research was funded by the National Social Science Foundation Project: Research on the Inheritance and Innovation of Miao Folk Songs in Contemporary China (20BMZ088) and the Research on the Cultivation Mode Reform of Chinese MFA in the New Era (2021JGB059), and Graduate Education and Teaching Reform Research Project of Central South University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.1028934/full#supplementary-material
Alam, M., Roongpisuthipong, W., Kim, N., Goyal, A., Swary, J., Brindise, R., et al. (2016). Utility of recorded guided imagery and relaxing music in reducing patient pain and anxiety, and surgeon anxiety, during cutaneous surgical procedures: A single-blinded randomized controlled trial. J. Am. Acad. Dermatol. 75, 585–589. doi: 10.1016/j.jaad.2016.02.1143
Al-Jubouri, M., Isam, S., Hussein, S., and Machuca-Contreras, F. (2021). Recitation of quran and music to reduce chemotherapy-induced anxiety among adult patients with cancer: A clinical trial. Nurs. Open. 8, 1606–1614. doi: 10.1002/nop2.781
Bulfone, T., Quattrin, R., Zanotti, R., Regattin, L., and Brusaferro, S. (2009). Effectiveness of music therapy for anxiety reduction in women with breast cancer in chemotherapy treatment. Holist. Nurs. Pract. 23, 238–242. doi: 10.1097/HNP.0b013e3181aeceee
Chen, L., Wang, T., Shih, Y., and Wu, L. (2013). Fifteen-minute music intervention reduces pre-radiotherapy anxiety in oncology patients. Eur. J. Oncol. Nurs. 17, 436–441. doi: 10.1016/j.ejon.2012.11.002
Danhauer, S., Vishnevsky, T., Campbell, C., McCoy, T., Tooze, J., Kanipe, K., et al. (2010). Music for patients with hematological malignancies undergoing bone marrow biopsy: A randomized controlled study of anxiety, perceived pain, and patient satisfaction. J. Soc. Integr. Oncol. 8, 140–147.
Firmeza, M., Rodrigues, A., Melo, G., Aguiar, M., Cunha, G., Oliveira, P., et al. (2017). Control of anxiety through music in a head and neckoutpatient clinic: A randomized clinical trial. Rev. Esc. Enferm. USP 51:e03201. doi: 10.1590/s1980-220x2016030503201
Giovagnoli, A., Manfredi, V., Parente, A., Schifano, L., Oliveri, S., and Avanzini, G. (2017). Cognitive training in Alzheimer’s disease: A controlled randomized study. Neurol. Sci. 38, 1485–1493. doi: 10.1007/s10072-017-3003-9
Higgins, J., Altman, D., Gøtzsche, P., Jüni, P., Moher, D., Oxman, A., et al. (2011). The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928. doi: 10.1136/bmj.d5928
Higgins, J., and Thompson, S. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558. doi: 10.1002/sim.1186
Kwekkeboom, K. (2003). Music versus distraction for procedural pain and anxiety in patients with cancer. Oncol. Nurs. Forum. 30, 433–440. doi: 10.1188/03.ONF.433-440
Lee, M., Huang, C., Lee, C., Kuo, T., Fang, Y., Chin-Hung Chen, V., et al. (2021). Investigation of anxiety and depressive disorders and psychiatric medication use before and after cancer diagnosis. Psychooncology 30, 919–927. doi: 10.1002/pon.5672
Li, X., Zhou, K., Yan, H., Wang, D., and Zhang, Y. (2012). Effects of music therapy on anxiety of patients with breast cancer after radical mastectomy: A randomized clinical trial. J. Adv. Nurs. 68, 1145–1155. doi: 10.1111/j.1365-2648.2011.05824.x
Li, Y., Xing, X., Shi, X., Yan, P., Chen, Y., Li, M., et al. (2020). The effectiveness of music therapy for patients with cancer: A systematic review and meta-analysis. J. Adv. Nurs. 76, 1111–1123. doi: 10.1111/jan.14313
Lin, M., Hsieh, Y., Hsu, Y., Fetzer, S., and Hsu, M. C. (2011). A randomised controlled trial of the effect of music therapy and verbal relaxation on chemotherapy-induced anxiety. J. Clin. Nurs. 20, 988–999. doi: 10.1111/j.1365-2702.2010.03525.x
Linden, W., Vodermaier, A., Mackenzie, R., and Greig, D. (2012). Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 141, 343–351. doi: 10.1016/j.jad.2012.03.025
Mausbach, B., Decastro, G., Schwab, R., Tiamson-Kassab, M., and Irwin, S. (2020). Healthcare use and costs in adult cancer patients with anxiety and depression. Depress. Anxiety 37, 908–915. doi: 10.1002/da.23059
Mishra, K., Jesse, E., Bukavina, L., Sopko, E., Arojo, I., Fernstrum, A., et al. (2022). Impact of music on postoperative pain. anxiety, and narcotic use after robotic prostatectomy: A randomized controlled trial. J. Adv. Pract. Oncol. 13, 121–126. doi: 10.6004/jadpro.2022.13.2.3
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Nguyen, K., Xiao, J., Chan, D., Zhang, M., and Chan, C. (2022). Effects of music intervention on anxiety, depression, and quality of life of cancer patients receiving chemotherapy: A systematic review and meta-analysis. Support. Care Cancer 30, 5615–5626. doi: 10.1007/s00520-022-06881-2
Nightingale, C., Rodriguez, C., and Carnaby, G. (2013). The impact of music interventions on anxiety for adult cancer patients: A meta-analysis and systematic review. Integr. Cancer Ther. 12, 393–403. doi: 10.1177/1534735413485817
O’Callaghan, C., Sproston, M., Wilkinson, K., Willis, D., Milner, A., Grocke, D., et al. (2012). Effect of self-selected music on adults’ anxiety and subjective experiences during initial radiotherapy treatment: A randomised controlled trial and qualitative research. J. Med. Imaging Radiat. Oncol. 56, 473–477. doi: 10.1111/j.1754-9485.2012.02395.x
O’Steen, L., Lockney, N., Morris, C., Johnson-Mallard, V., Pereira, D., and Amdur, R. J. A. (2021). Prospective randomized trial of the influence of music on anxiety in patients starting radiation therapy for cancer. Int. J. Radiat. Oncol. Biol. Phys. 109, 670–674. doi: 10.1016/j.ijrobp.2020.09.048
Pacchetti, C., Mancini, F., Aglieri, R., Fundarò, C., Martignoni, E., and Nappi, G. (2000). Active music therapy in Parkinson’s disease: An integrative method for motor and emotional rehabilitation. Psychosom. Med. 62, 386–393. doi: 10.1097/00006842-200005000-00012
Rossetti, A., Chadha, M., Torres, B., Lee, J., Hylton, D., Loewy, J., et al. (2017). The impact of music therapy on anxiety in cancer patients undergoing simulation for radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 99, 103–110. doi: 10.1016/j.ijrobp.2017.05.003
Shabanloei, R., Golchin, M., Esfahani, A., Dolatkhah, R., and Rasoulian, M. (2010). Effects of music therapy on pain and anxiety in patients undergoing bone marrow biopsy and aspiration. AORN J. 91, 746–751. doi: 10.1016/j.aorn.2010.04.001
Simavli, S., Kaygusuz, I., Gumus, I., Usluogulları, B., Yildirim, M., and Kafali, H. (2014). Effect of music therapy during vaginal delivery on postpartum pain relief and mental health. J. Affect. Disord. 156, 194–199. doi: 10.1016/j.jad.2013.12.027
Tola, Y., Chow, K., and Liang, W. (2021). Effects of non-pharmacological interventions on preoperative anxiety and postoperative pain in patients undergoing breast cancer surgery: A systematic review. J. Clin. Nurs. 30, 3369–3384. doi: 10.1111/jocn.15827
Vachiramon, V., Sobanko, J., Rattanaumpawan, P., and Miller, C. (2013). Music reduces patient anxiety during Mohs surgery: An open-label randomized controlled trial. Dermatol. Surg. 39, 298–305. doi: 10.1111/dsu.12047
Wang, Y., Li, J., Shi, J., Que, J., Liu, J., Lappin, J., et al. (2020). Depression and anxiety in relation to cancer incidence and mortality: A systematic review and meta-analysis of cohort studies. Mol. Psychiatry 25, 1487–1499. doi: 10.1038/s41380-019-0595-x
Wren, A., Shelby, R., Soo, M., Huysmans, Z., Jarosz, J., and Keefe, F. (2019). Preliminary efficacy of a lovingkindness meditation intervention for patients undergoing biopsy and breast cancer surgery: A randomized controlled pilot study. Support. Care Cancer 27, 3583–3592. doi: 10.1007/s00520-019-4657-z
Wu, Z., Kong, L., and Zhang, Q. (2022). Research progress of music therapy on gait intervention in patients with Parkinson’s disease. Int. J. Environ. Res. Public Health 19:9568. doi: 10.3390/ijerph19159568
Zhao, K., Bai, Z., Bo, A., and Chi, I. (2016). A systematic review and meta-analysis of music therapy for the older adults with depression. Int. J. Geriatr. Psychiatry 31, 1188–1198. doi: 10.1002/gps.4494
Zhou, K., Li, X., Li, J., Liu, M., Dang, S., Wang, D., et al. (2015). A clinical randomized controlled trial of music therapy and progressive muscle relaxation training in female breast cancer patients after radical mastectomy: Results on depression, anxiety and length of hospital stay. Eur. J. Oncol. Nurs. 19, 54–59. doi: 10.1016/j.ejon.2014.07.010
Keywords: music, music therapy, mental health, cancer, meta-analysis
Citation: Zang L, Cheng C, Zhou Y and Liu X (2023) Music therapy effect on anxiety reduction among patients with cancer: A meta-analysis. Front. Psychol. 13:1028934. doi: 10.3389/fpsyg.2022.1028934
Received: 26 August 2022; Accepted: 01 December 2022;
Published: 06 January 2023.
Edited by:
Peng Wang, Anhui Medical University, ChinaReviewed by:
Fatemeh Khademi, Arak University of Medical Sciences, IranCopyright © 2023 Zang, Cheng, Zhou and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuemei Liu,  bGl1eG1AY3N1LmVkdS5jbg==
bGl1eG1AY3N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.